Javier Cabo Salvador
Medical Doctor and Doctor in Cardiovascular Surgery
The different forms of computational science, whether descriptive, diagnostic, predictive, prescriptive, or preventive, are helpful in creating predictive models based on regression techniques like linear regression, discrete choice, time series, classification trees, Machine Learning and Data Mining methods like Gradient Boosting, Random Forest, and Bagging used to produce decision tree models, as well as plus “Bayesian Analysis” and “Artificial Neural Networks”.
These tools can be used to combine learning models and improve overall results by analysing and relating large blocks of data (data mining) to extract patterns and significant trends and in that way create “decision models” based on such methods as “system dynamics”, developed at MIT. Table 1.
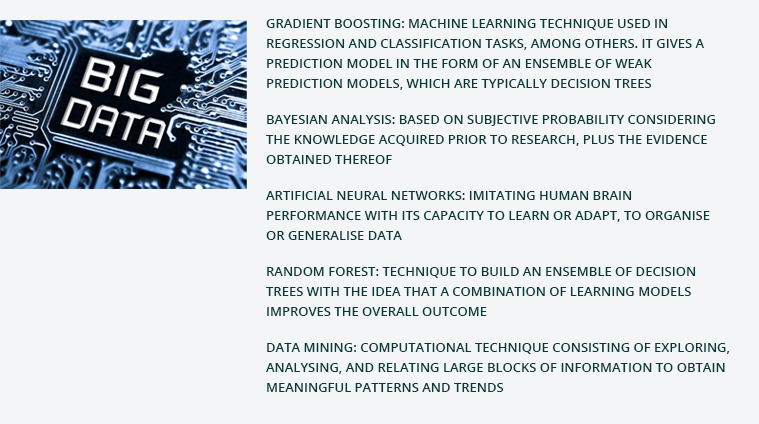
Table 1. Predictive analytics methods used to generate decision models.
Source: By the autor.
These methods allow us to analyse and model behaviour over time in complex chaotic systems like the human body and to describe the relationships among all the decision elements and thus be able to use large numbers of variables and structural data to predict outcomes and arrive at more objective decisions with greater certainty.
In medicine generally and in cardiovascular medicine in particular, “predictive analytics” are extremely helpful in deciding which patients are at risk of developing certain pathological conditions or cardiovascular diseases (CVDs) and in providing a basis for decision-making when choosing among the various treatment and care options.
Predictive analytics tools are important to be able to implement preventive measures to keep dangerous cardiovascular conditions, the most common cause of death worldwide, from developing and in that way reduce health insurance claim rates.
Cardiovascular diseases have far-reaching social (mortality and morbidity statistics) and economic (public healthcare costs) impact. Even so, their great importance and social repercussions notwithstanding, most citizens in the European Union (EU) are not yet mindful of the potentially fatal impact of heart disease on the populace.
A recent survey conducted by Daichi Sankyo, a Japanese pharmaceutical company, in the framework of the We Care for Every Heartbeat campaign, in five European countries (United Kingdom, Italy, Germany, Spain, and the Netherlands) assessed the level of awareness and understanding of cardiovascular diseases and their impact on society by the general population. The survey results show that on average only 24% of respondents knew that cardiovascular disease was the leading cause of death in Europe. This figure fell to 19% in Spain, the country in this study with the least awareness of the potential impact of heart disease on mortality.
According to data reported by the World Health Organization (WHO), the ten main causes of mortality worldwide in the most recent period on record, 2019 and 2020, were, in order of rank:
CVDs accounted for the top two, first myocardial ischaemia (heart attack), followed by neurovascular disorders (ischaemic or haemorrhagic stroke). Third was lung disease, first chronic obstructive lung disease (COPD), followed by respiratory infections; neonatal mortality; tracheal, bronchial, and lung cancers; Alzheimer's disease and other dementias; digestive disorders producing diarrhoea; diabetes mellitus; and ranked tenth, kidney disease (Figure 1).
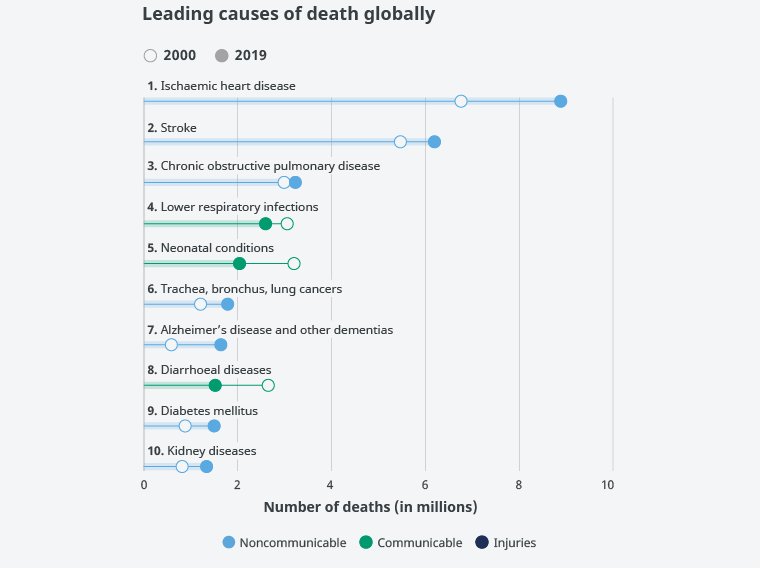
Figure 1. Leading causes of death worldwide.
Source: World Health Organization.
The 10 main causes of death accounted for 55% of the 55.4 million deaths worldwide in 2019. These leading causes of death worldwide have been divided into three main categories based on the total number of lives lost: cardiovascular diseases (ischaemic heart disease, stroke), respiratory diseases (chronic obstructive lung disease, lower respiratory tract infections), and neonatal conditions including asphyxia and birth trauma, sepsis and neonatal infections, and preterm birth complications. Causes of death can be grouped into three categories, communicable diseases (infectious and parasitic diseases, maternal, perinatal, and nutritional conditions), noncommunicable diseases (chronic), and injuries.
Worldwide, in 2019 7 of the 10 main causes of death were noncommunicable diseases. These 7 causes accounted for 44% of all deaths and 80% of all deaths from the 10 leading causes. All noncommunicable diseases together accounted for 74% of deaths globally in 2019. Ischaemic heart disease is the main cause of death, accounting for 16% of total deaths. This disease has been responsible for the largest increase in deaths since the year 2000, rising from 2 million deaths in 2000 to 8.9 million deaths in 2019. Stroke and chronic obstructive lung disease are the second and third leading causes of death and account for approximately 11% and 6% of all deaths, respectively.
Lower respiratory tract infections are still the deadliest communicable disease in the world and are the fourth leading cause of death. However, the number of deaths has gone down considerably, taking 2.6 million lives in 2019, 460,000 fewer than in 2000. Neonatal conditions rank fifth. Deaths from neonatal causes are one of the categories in which deaths have fallen the most in absolute terms over the past two decades. These conditions took the lives of 2 million newborns and infants in 2019, that is, 1.2 million fewer than in 2000.
Deaths from noncommunicable diseases are on the rise. Deaths from tracheal, bronchial, and lung cancers have risen from 1.2 million to 1.8 million and now rank sixth among the leading causes of death. Alzheimer's disease and other forms of dementia were the seventh leading cause of death in 2019 and disproportionately affect women. Women make up 65% of deaths from Alzheimer's and other forms of dementia. Diarrhoeal diseases have undergone one of the largest declines in number of deaths, dropping from 2.6 million deaths in 2000 to 1.5 million deaths in 2019 worldwide. Diabetes has turned into one of the 10 leading causes of death following an appreciable percentage increase of 70% since the year 2000. Of the 10 main causes of death, diabetes is also behind the largest increase in deaths in men, rising by 80% since 2000.
Other diseases that were among the 10 leading causes of death in 2000 are no longer on the list. HIV/AIDS is one of these. Deaths from HIV/AIDS have fallen by 51% in the last 20 years, and this cause has dropped from being the eighth-ranked cause worldwide in 2000 to nineteenth place in 2019. Deaths from kidney disease have increased, and this cause has risen from the 13th cause of death to tenth worldwide. Deaths from this cause rose from 813,000 people in 2000 to 1.3 million in 2019.
The World Bank classifies the world's economies into four income groups based on gross national income – low, lower-middle, upper-middle, and high. Breaking down reported mortality by country shows that the causes of death differ somewhat according to countries' level of development and GDP (Figure 2).
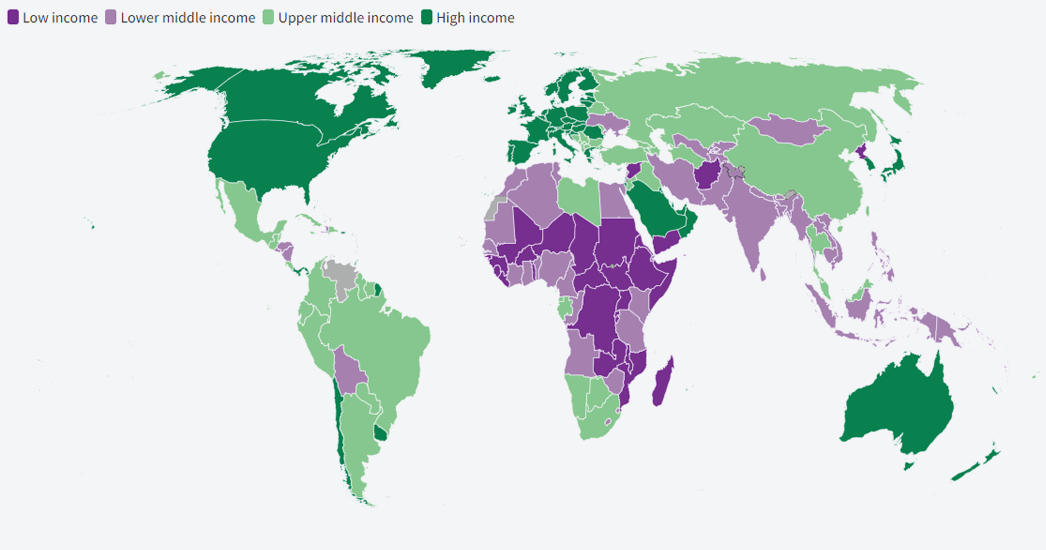
Figure 2. Country ranking by income level (2021).
Source: World Bank.
The main causes of death in low-GDP, low-income, less socially and economically developed countries are neonatal mortality ranking first, followed by respiratory infections in second place, and then the CVDs ischaemic heart disease ranking third and stroke ranking fourth. Next in order of frequency come diarrhoeal diseases, malaria, traffic accidents, tuberculosis, HIV/AIDS, and cirrhosis of the liver (Figure 3).
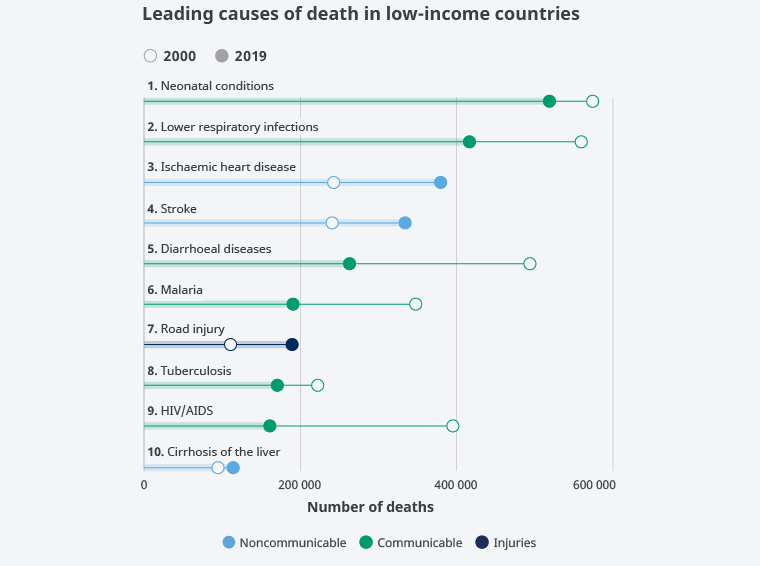
Figure 3. Main causes of death in low-income countries.
Source: World Health Organization.
According to WHO statistics, people living in low-income countries are far more likely to die from a communicable disease than from a noncommunicable disease. Despite a global decline in communicable diseases, they still account for 6 of the top 10 causes of death in low-income countries. Malaria, tuberculosis, and HIV/AIDS continue in the top 10 leading causes of death. Nevertheless, all three are declining considerably. Among the top 10 causes of death in this group, HIV/AIDS has decreased the most, with 59% fewer deaths in 2019 than in 2000, or 161,000 and 395,000 people, respectively. Diarrhoeal diseases are more significant as a cause of death in low-income countries, ranking among the five main causes of death in this income group. Still, diarrhoeal diseases in low-income countries are decreasing, with the second largest decline in fatalities among the top 10 causes (231,000 fewer deaths). Deaths from chronic obstructive pulmonary disease are especially infrequent in low-income countries compared to the countries in the other income groups. It is not one of the 10 leading causes of death in low-income countries, yet it ranks as one of the top 5 causes in the countries in all other income groups.
Lower-middle-income countries have the most disparate main causes of death: five noncommunicable, four communicable diseases, and injuries. Diabetes is a growing cause of death in this income group, rising from the 15th to the 9th leading cause of death. The number of deaths from this disease have nearly doubled since 2000.
Diarrhoeal diseases remain a significant challenge as one of the 10 leading causes of death in the countries in this income group. However, this category of diseases has experienced the biggest decrease in absolute numbers of deaths, from 1.9 million to 1.1 million between 2000 and 2019. The biggest increase in deaths in absolute numbers has been for ischaemic heart disease, with deaths rising by more than 1 million to 3.1 million since 2000. Among the 10 main causes of death, HIV/AIDS has dropped the most in the ranking since 2000, falling from 8th to 15th.
Thus, CVDs are now clearly the two main causes of death in the lower-middle-income countries. Myocardial ischaemia (heart attack) is the leading cause of death and stroke the second leading cause, followed by neonatal mortality, lung diseases (COPD and respiratory infections), diarrhoeal diseases, tuberculosis, cirrhosis of the liver, diabetes mellitus, and traffic accidents (Figure 4).
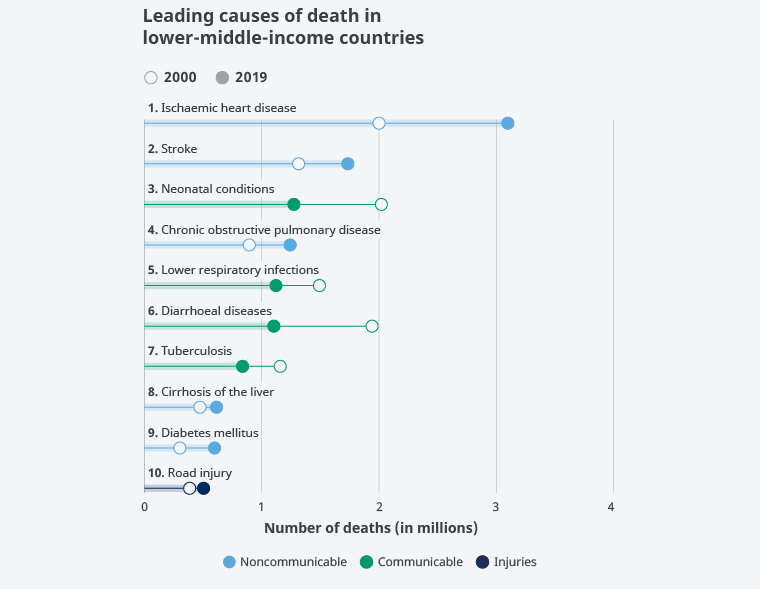
Figure 4. Main causes of death in lower-middle-income countries.
Source: World Health Organization.
According to WHO data, in the upper-middle-income countries there has been a notable rise in deaths from lung cancer, increasing by 411,000, more than twice the increase in deaths in all the other three income group countries combined. Stomach cancer features highly in upper-middle-income countries compared to the other country income groups. These countries are the only group in which this disease is one of the 10 main causes of death.
One of the biggest decreases in deaths in absolute terms is from chronic obstructive pulmonary disease, falling by some 264,000, to 1.3 million deaths. However, deaths from ischaemic heart disease have grown by more than 1.2 million, the largest increase in deaths from this cause, in absolute numbers, in any country income group. There is only one communicable disease (lower respiratory tract infections) among the 10 leading causes of death in upper-middle-income countries. At the same time, there has been a 31% drop in deaths from suicide since 2000 in the countries in this income group, falling to 234,000 deaths in 2019.
In short, cardiovascular diseases, i.e., myocardial ischaemia (heart attack), stroke, and hypertensive heart disease, rank first, second, and seventh as causes of death in the upper-middle-income countries. Respiratory diseases (COPD, tracheal, bronchial, and lung cancers, and respiratory infections) rank third, fourth, and fifth as causes of death, followed by diabetes, hypertensive heart disease, Alzheimer's disease and dementias, stomach cancer, and traffic accidents. Neonatal mortality and diarrhoeal diseases have disappeared as main causes of death in these countries (Figure 5).
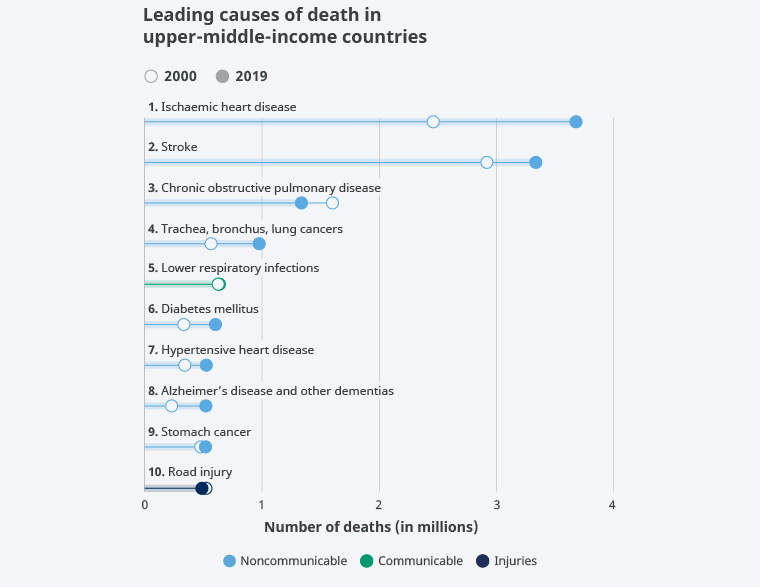
Figure 5. Main causes of death in upper-middle-income countries.
Source: World Health Organization.
Deaths from all but 2 of the 10 main causes of death have been rising in high-income countries. Ischaemic heart disease and stroke are the only causes of death in the top 10 for which the total numbers have gone down between 2000 and 2019, by 16% (or 327,000 deaths) and by 21% (or 205,000 deaths) respectively. High-income countries are the only income group in which deaths from these two diseases have been falling.
In any case, ischaemic heart disease and stroke are still among the three main causes of death in the countries in this income group, with a combined total of over 2.5 million fatalities in 2019. In addition, deaths from hypertensive heart disease are on the rise. Mirroring a worldwide trend, this disease has climbed from being the 18th leading cause of death to being the 9th. Deaths from Alzheimer's disease and other dementias have increased, overtaking stroke to become the second leading cause of death in high-income countries, where these conditions were responsible for the deaths of 814,000 people in 2019. And as in the case of upper-middle-income countries, there is only one communicable disease among the 10 main causes of death, lower respiratory tract infections.
To sum up, in highly developed, high-income countries, the top three main causes of death are, first, CVD (heart attack), second, Alzheimer's and other dementias, and third, another CVD, stroke. Ranked fourth through sixth are respiratory diseases, e.g., tracheal, bronchial, and lung cancers, COPD, and respiratory infections. They are followed by colorectal cancer in seventh place, kidney disease in eighth place, with another cardiovascular disease condition, hypertensive heart disease, ranked ninth, and finally diabetes ranked tenth (Figure 6).
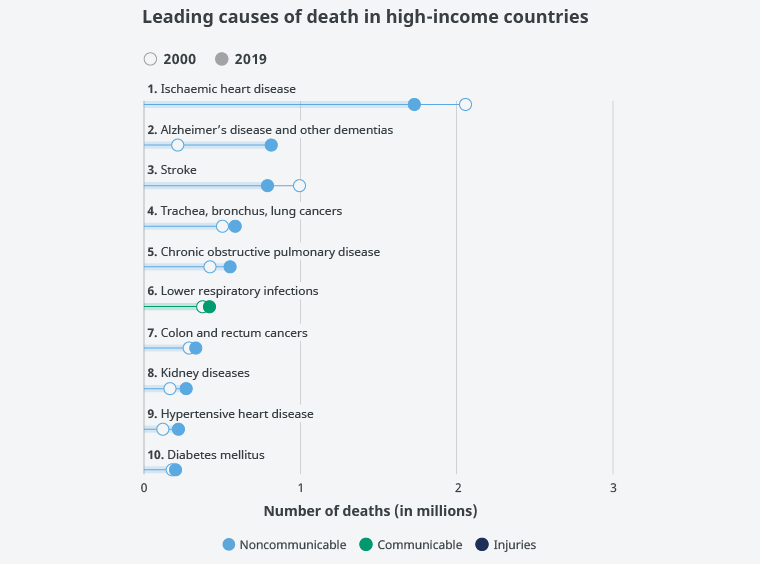
Figure 6. Main causes of death in high-income countries.
Source: World Health Organization.
It should be noted that mortality from cardiovascular disease, the main cause of death worldwide, can be seen to have increased by 25.1% overall. This increase has been most pronounced in the countries of Southeast Asia (56.2%), in the countries of the eastern Mediterranean region (54.1%), in the countries of the western Pacific (47.4%), in the African countries (31.4%), and in the countries of the Americas (14.9%). In contrast, a 14% decrease in reported mortality has been observed in Europe (Figure 7).
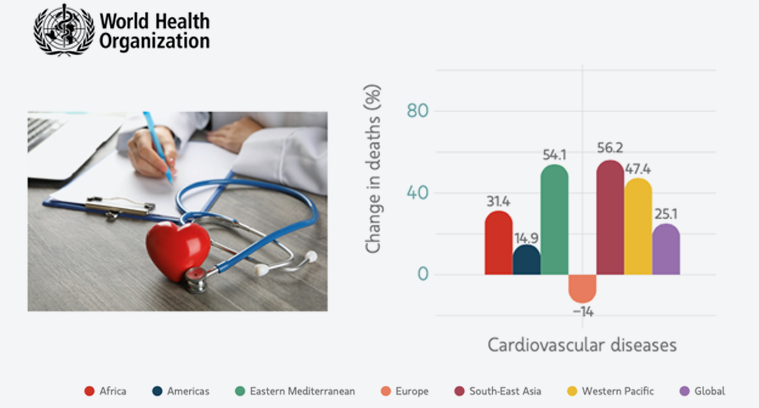
Figure 7. Increased mortality from cardiovascular disease. 2019-2020.
Source: World Health Organization.
Therefore, ischaemic heart disease is the leading cause of death worldwide, accounting for 16% of all fatalities globally since the year 2000, with deaths from this cause growing the most, rising by over 2 million, to 8.9 million deaths in 2019.
According to Eurostat, the main causes of death in all European countries are cardiovascular disease, ischaemic heart disease (heart attack), and stroke, followed by cancer, especially colorectal and lung cancer (Table 2 and Figure 8).
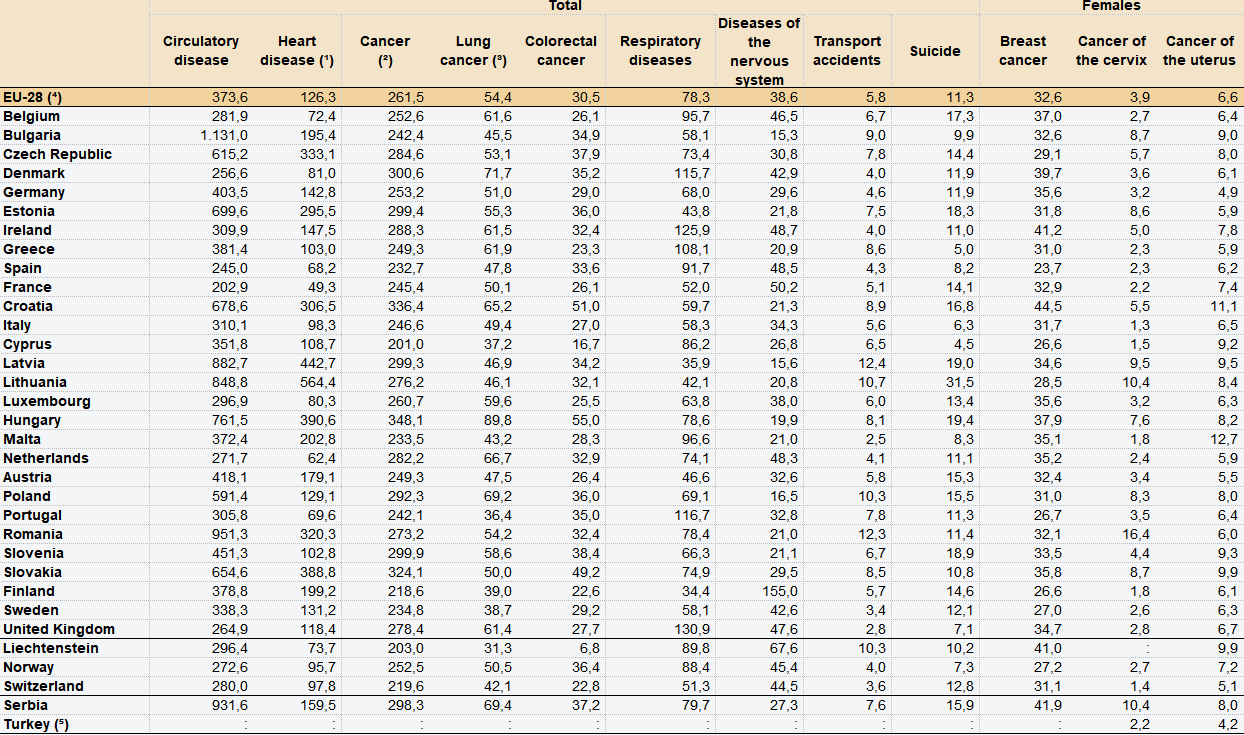
Table 2. Main causes of death in Europe by country.
Source: Eurostat.
Circulatory diseases like ischaemic heart disease (heart attack) and cerebrovascular conditions like stroke are the most common causes of death. Ischaemic heart disease was responsible for 126 deaths per 100,000 inhabitants in the EU based on 2014 data.
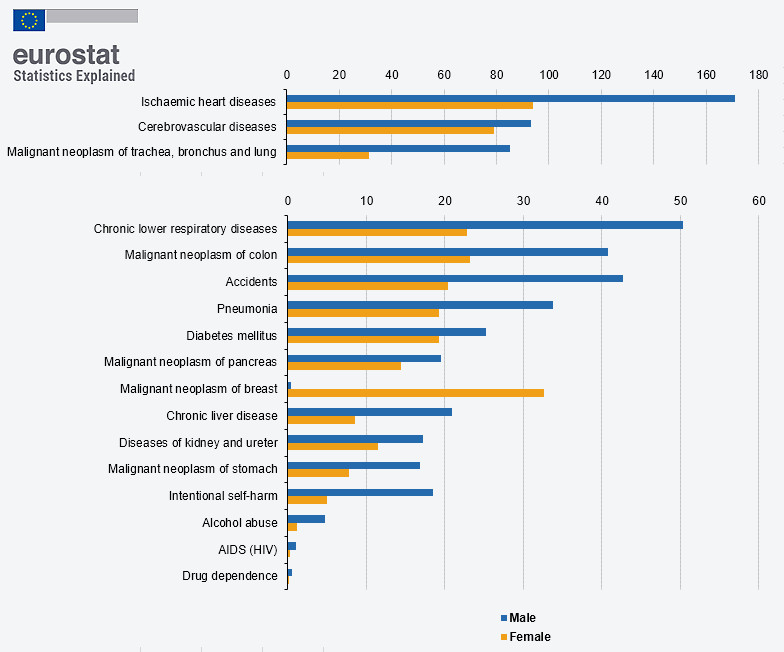
Figure 8. Main causes of death in Europe.
Source: Eurostat.
There are nearly 4 million deaths from cardiovascular disease (CVD) in Europe per year, i.e., 10,000 deaths daily. Prevalence is therefore extremely high. Most recently, more than 60 million people were living with CVD in the EU in 2020, and nearly 13 million new cases are diagnosed each year. Based on longevity and life expectancy projections, incidence is expected to increase in the coming years. Ischaemic heart disease alone was responsible for 126 deaths per 100,000 inhabitants in the EU and for 16% of deaths worldwide.
The standardised average mortality rate from heart disease in Spain in 2020 was 219.4 deaths per 100,000 inhabitants. It was the most frequent cause of death at 24.30%, followed by cancer at 22.80%. It is noteworthy that the mortality rate in women (53.32%) was higher than the rate recorded for men (46.67%) (Figure 9).
![Figure 9. Causes of death in Spain. Source: Instituto Nacional de Estadística [Spain's National Institute of Statistics] and Sociedad Española de Cardiología [Spanish Cardiology Association].](../../../../../almacen/numero18/ENG/analisis_figura_9_en.png)
Figure 9. Causes of death in Spain.
Source: Instituto Nacional de Estadística [Spain's National Institute of Statistics] and Sociedad Española de Cardiología [Spanish Cardiology Association].
In absolute numbers of cases per year, deaths from CVD in 2020 (119,853 deaths) increased compared to deaths from that same cause in 2019 (116,215 deaths), a 2.4% rise. Again, it should be noted that according to the data, nearly 8,000 more women than men die from CVD in Spain each year (Figure 10).
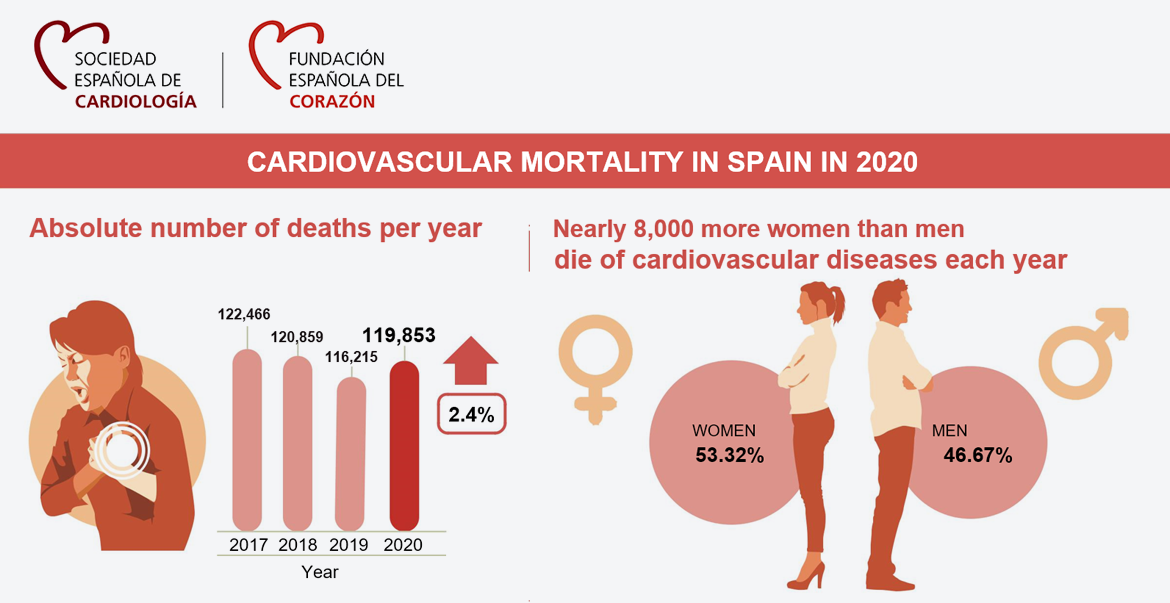
Figure 10. Deaths from CVD in Spain.
Source: Sociedad Española de Cardiología and Instituto Nacional de Estadística.
Circulatory diseases remain the leading cause of death in Spain. In 2020 119,853 people died from cardiovascular causes, 24.3% of all deaths. At 112,741 deaths (22.8%), tumours were the second cause of death, and infectious diseases, including COVID-19, were the third cause of death, at 80,796 fatalities (16.4%).
Based on data from Spain's regions, the standardised average mortality rate from CVD in 2020 was 219.4 deaths per 100,000 inhabitants. The Autonomous Cities, Ceuta at 321.6 deaths per 100,000 inhabitants and Melilla at 298.5 deaths per 100,000 inhabitants, had the highest rates in the entire country. By Autonomous Community, Andalusia (282.3 deaths), Murcia (260.9 deaths), and Extremadura (245.4 deaths) were the regions with the most deaths from circulatory diseases. Four other regions (Valencia, Asturias, the Canary Islands, and Castilla-La Mancha) had standardised mortality rates from cardiovascular causes that were higher than average. A total of 10 Autonomous Communities had standardised mortality rates from heart disease that were lower than average. Navarre (172.8), Madrid (173.2), and the Basque Country (186.3) were the regions with the lowest death rates from circulatory disease in Spain (Figure 11).
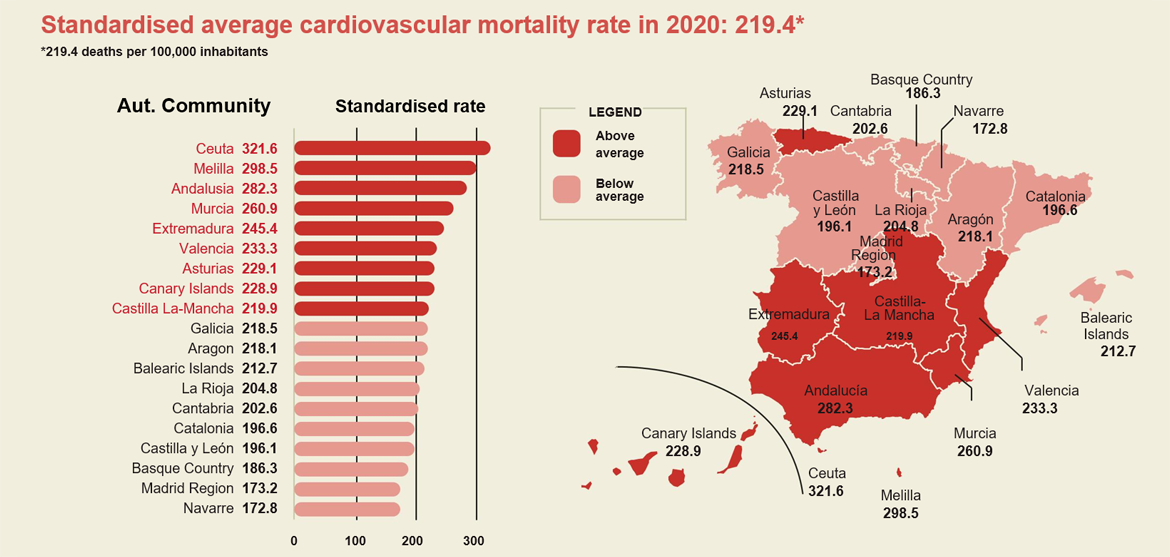
Figure 11. Standardised average mortality rates from CVD in Spain in 2020 by Autonomous Community.
Source: Instituto Nacional de Estadística.
The number of deaths from hypertensive heart disease in Spain in 2020 (14,271) rose compared with the previous year (11,854). Mortality from this cause has been growing non-stop over the past 15 years, to the point where today the number of deaths from this cause doubles the number of 2006. Mortality from stroke has decreased (Figure 12).
However, in connection with this decrease in mortality from cerebrovascular causes, the 70th annual meeting of the Sociedad Española de Neurología [Spanish Neurology Society] said that the number of cases of stroke and mortality caused by stroke are set to grow by 35% over the next 15 years.
At the present time, there are 120,000 new cases of stroke and 27,000 people die from this cause in Spain each year. It is the leading cause of death in women, the third leading cause of death in men, and the main cause of acquired disability in adults. In Spain two of every three people who have suffered a stroke are older than 65 years of age, but the number of cases among people aged between 20 and 64 has risen by 25% in the past 20 years. The most important aspect to bear in mind is that at least 80% of strokes could be avoided by taking appropriate preventive measures to address the risk factors associated with this disease, e.g., high blood pressure, diabetes mellitus, smoking, and hyperlipidaemia, along with related lifestyle factors like obesity, improper eating habits and nutrition, and physical inactivity. These risk factors are also associated with mortality from cardiovascular ischaemia (heart attack) and non-ischaemic heart disease (arrhythmias and sudden death) (Figure 12).
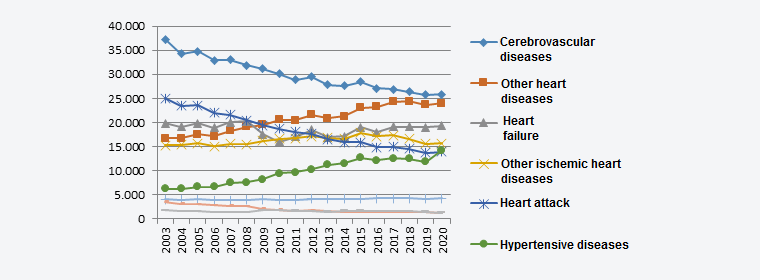
Figure 12. Time trend for causes of death in Spain from 2003 to 2020.
Source: Instituto Nacional de Estadística.
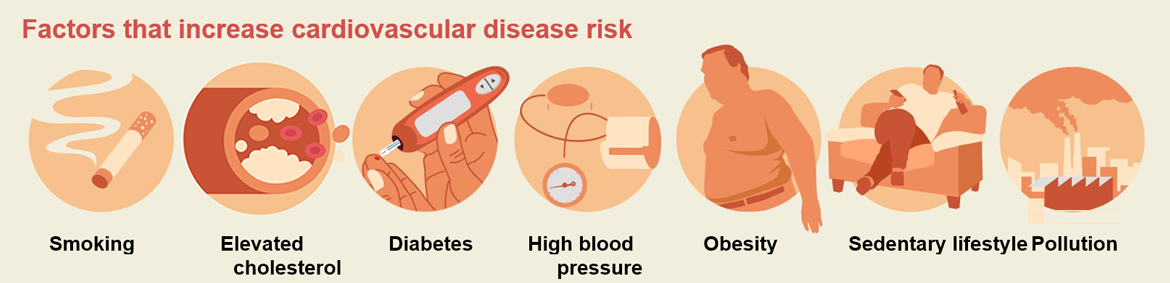
Figure 13. Factors for heightened risk of cardiovascular heart disease and associated death.
Source: Instituto Nacional de Estadística and Sociedad Española de Cardiología.
Two of the main cardiovascular risk factors that trigger ischaemic heart disease and ischaemic stroke are elevated cholesterol, more specifically LDL (low-density lipoprotein) cholesterol, and hypertension. They can be readily altered by changes in eating habits and lifestyle, in certain cases in association with treatment with statins and/or vasopressors or beta blockers.
Worldwide, the American Heart Association, the European Society of Cardiology, and other international scientific groups have developed consensus guidelines for preventive action for both ischaemic heart disease (heart attack) and cerebral ischaemia (ischaemic stroke). One of these is the "Framingham risk score", from the United States, used to assess the probability that coronary morbidity or mortality (angina, heart attack, sudden death) will occur in the next 10 years based on age, blood pressure, and cholesterol level.
Additional tools connected with cardiovascular risk include the "SCORE chart" in Europe for calculating mortality from CVD (coronary and cerebrovascular); the "Reynolds risk score", also from the United States, for assessing cardiovascular risk (cardiovascular mortality, heart attack, revascularisation, and stroke) based on age, blood pressure, cholesterol level, diabetes, and C-reactive protein; the "QRISK calculator" from the United Kingdom for calculating the probability of CVD morbidity and mortality (coronary and cerebrovascular) based on age, blood pressure, cholesterol level, and body mass index.
Two further calculators are the "ASSIGN score" from Scotland for assessing CVD mortality and coronary morbidity (hospitalisation and revascularisation) based on age, blood pressure, and cholesterol level; and the "PROCAM study" in Germany for calculating coronary morbidity and mortality (angina, heart attack, sudden death) based on age, blood pressure, cholesterol level, diabetes, and triacylglycerols.
Lastly, there is the "CHA2DS2-VASc score", prediction rules for stroke prevention in patients with atrial fibrillation using oral anticoagulation therapy (Table 3).
The most commonly used risk stratification algorithms
![Table 3. Most widely used risk stratification algorithms worldwide. Source: Revista Española de Cardiología [Spanish Journal of Cardiology]; Suppl. 2012; 12(C):8-11.](../../../../../almacen/numero18/ENG/analisis_tabla_3_eng.png)
Table 3. Most widely used risk stratification algorithms worldwide.
Source: Revista Española de Cardiología [Spanish Journal of Cardiology]; Suppl. 2012; 12(C):8-11.
The most widely used stratification algorithms include the Framingham risk score, developed based on a cohort of persons aged 30 to 62 in the United States and validated worldwide. It is used to assess the probability of coronary morbidity and mortality (angina, heart attack, sudden death) in the next 10 years based on age, both LDL and HDL cholesterol levels, blood pressure, presence or absence of diabetes mellitus, and smoking habit (Figure 14).
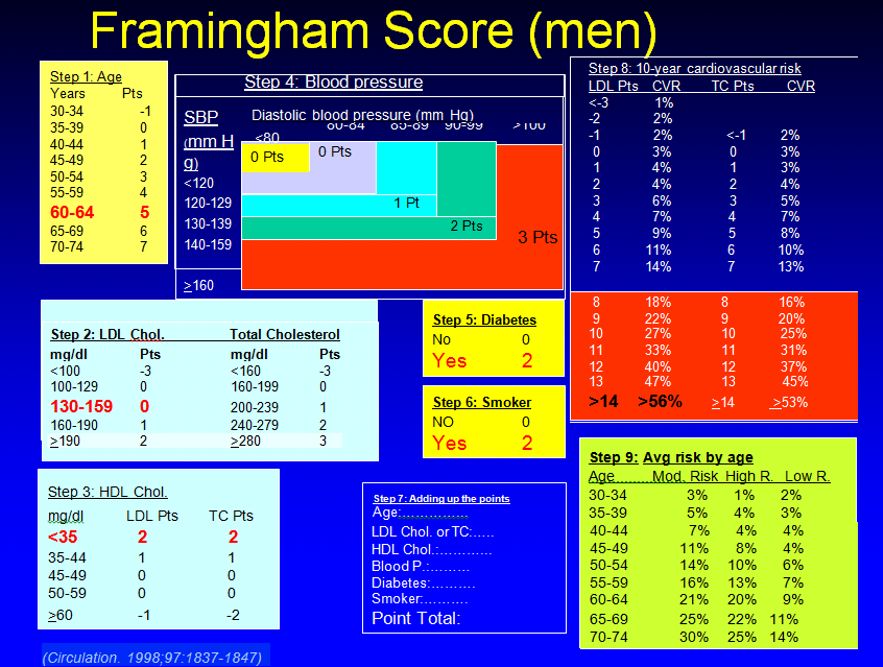
Figure 14. Exemplification of the Framingham risk score.
Source: Circulation. 1998; 97:1837.1847.
Another widely used algorithm in Europe, and hence in Spain, is the SCORE chart, developed based on a cohort of Europeans between the ages of 45 and 64 and validated on a broad sample cohort of Europeans. It assesses the risk of mortality from CVD (coronary and cerebrovascular) by applying 10-year cardiovascular mortality hazard ratios based on a series of variables including age, sex, systolic blood pressure, smoking habit, cholesterol (LDL and HDL), and prevalence of CVD in the population (Figure 15).
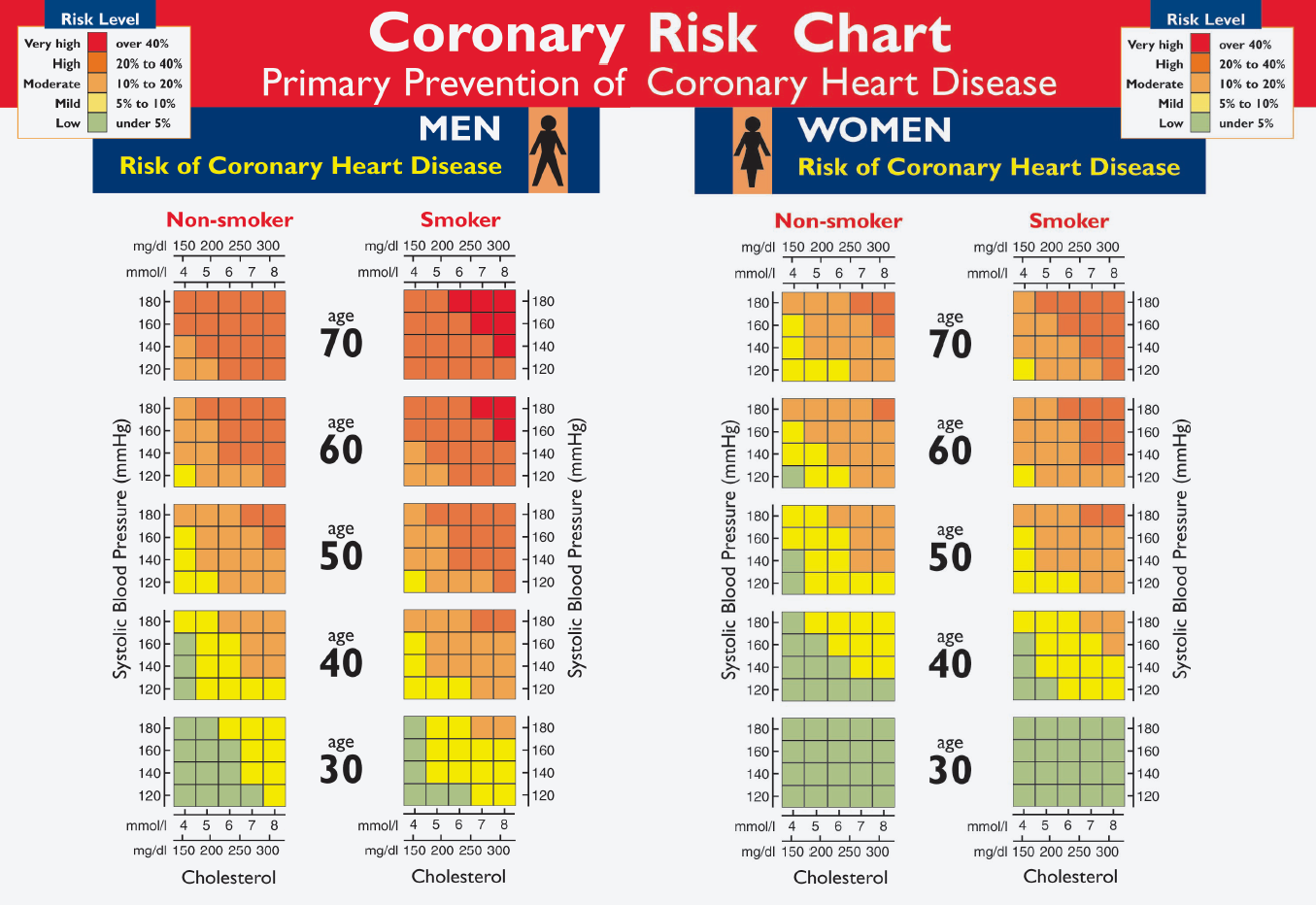
Figure 15. Exemplification of the SCORE chart.
Source: https://scielo.isciii.es/pdf/medif/v11n3/revision.pdf
The CHA2DS2-VASc score is another popular scale used in the interest of preventing cardiovascular disease, more specifically cerebrovascular causes of stroke in patients with arrhythmia (atrial fibrillation: AF). AF is the most common arrhythmia that has clinical repercussions. It is responsible for the most visits to emergency rooms and causes the most days spent in hospital. It is associated with increased morbidity (particularly stroke and heart failure) and mortality. AF grows more prevalent in both men and women with age. AF is increasingly being related not to the presence of existing heart disease but to a combination of cardiovascular risk factors closely linked to lifestyle, such as obesity, sedentary habits, diabetes mellitus, and sleep apnoea. AF is more prevalent in the developed countries, where an ageing population is combined with a sedentary lifestyle and obesity, than in the less developed countries. It affects 1-2% of the general population and is projected to increase in the coming years. Forecasts suggest that prevalence will at least double over the next 50 years.
According to studies in Europe, prevalence is estimated at between 0.2 and 2% of the general population and at between 1.5 and 5.5% of the population over 50. Available data suggest that prevalence is similar in the European countries and in the other developed countries, including Spain. Atrial fibrillation is the most frequent arrhythmia in the world, affecting 33 million people, or 0.5% of the global population.
There have been numerous European studies on the prevalence of AF in the different countries in our region. The Rotterdam Study is the most representative in Europe. The Rotterdam Study assesses the incidence and prevalence of AF in the population aged 55 and over. A total of 7,983 patients have been followed for around 7 years. AF prevalence was 5.5% of the total population, 0.7% of 55–59-year-olds and 17.8% of the over 85-year-olds. Other studies, like the FAMA Study in Portugal, have assessed the prevalence of AF in 10,447 randomly selected people over 40. Total prevalence was 2.5%, similar in both sexes, increasing with age. Another study carried out in France using diagnostic electrocardiograms on a population of 154,070 people 30 years and older found a prevalence of 0.05% in men under 50 and 0.01% in women under 50; in subjects 80 and over, prevalence was 6.5% in men and 5.2% in women.
The data from the Rotterdam Study have been used to estimate the population that could suffer from AF in the European Union from 2000 to 2060. It was estimated that there were 8.8 million adults with AF in Europe in 2010. If the prevalence of AF remains constant, this number will more than double and could reach 17.9 million by 2060. According to the Rotterdam Study results for the population 55 and over, total incidence was 9.9/1,000 persons/year, higher for men than for women. Incidence in the 55–59-year-old age group was 1.1/1,000 people/year, rising to 20.7/1,000 persons/year in the 80–84-year-old age group. A recent study of patients 45 and older in the United Kingdom observed an increase in standardised incidence of AF from 5.9 to 6.9/1,000 people/year over the past decade. Other recent studies on the general population recorded incidences of from 0.23/1,000 persons/year in Iceland to 0.41/1,000 persons/year in Germany to 0.9/1,000 persons/year in Scotland.
Overall incidence of AF in the general population worldwide was 60.7/100,000 persons/year for men and 43.8/100,000 persons/year for women in 1990. Estimated incidence was higher in 2010, 77.5/100,000 persons/year for men and 59.5/100,000 persons/year for women (Figure 16). Incidence was significantly higher (roughly double) in the developed countries compared to the developing countries. Applying these incidence rates to the global population in 2010 yielded an estimated 2.7 million new cases of AF in men and 2 million new cases in women each year. There are no prospective studies that can be used to estimate AF incidence in the general population in Spain.
Since AF is common in the elderly, prevalence can be expected to double, at least, in the next 2 or 3 decades. Considering that the prevalence of AF risk factors is also on the rise, this prediction is likely to fall short.
Atrial fibrillation
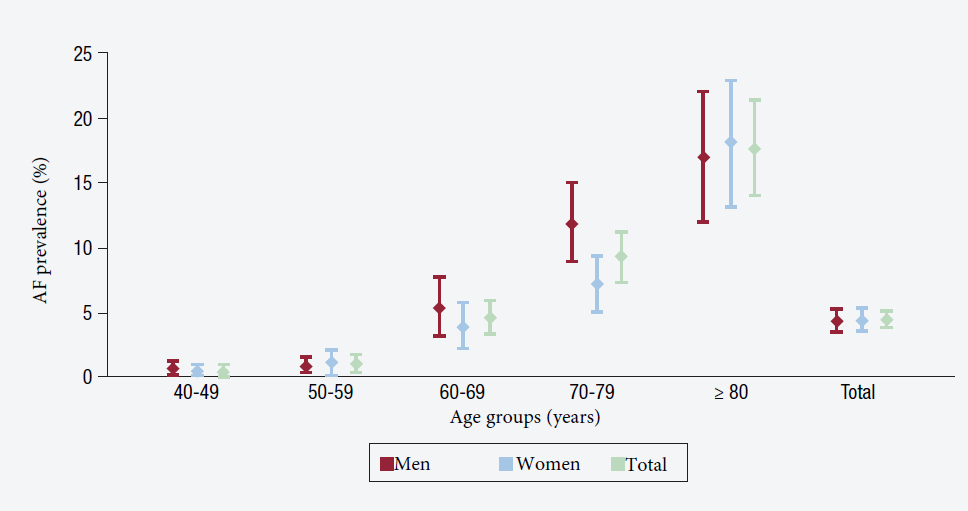
Figure 16. Prevalence of atrial fibrillation.
Source: Revista Española de Cardiología. 2016; 16 Suppl. A: 2-7.
AF is a serious arrhythmia with broad social repercussions. Current prevalence of atrial fibrillation in adults stands at approximately 2-4% but is expected to double or triple in the coming years as people live longer. AF increases mortality by a factor of 1.5-3.5 and the risk of stroke by a factor of 5 and is responsible for 20-30% of ischaemic strokes and 10% of cryptogenic strokes. Embolic stroke tends to be more severe than other types of strokes, with high rates of recurrence and permanent disability.
Furthermore, AF heightens the risk of dementia and causes functional impairment in most patients. It is estimated that approximately 30% of AF patients have to be hospitalised at least once every year. In fact, AF patients are at twice the risk of hospitalisation than patients without AF, particularly from cardiovascular causes (Figure 17).
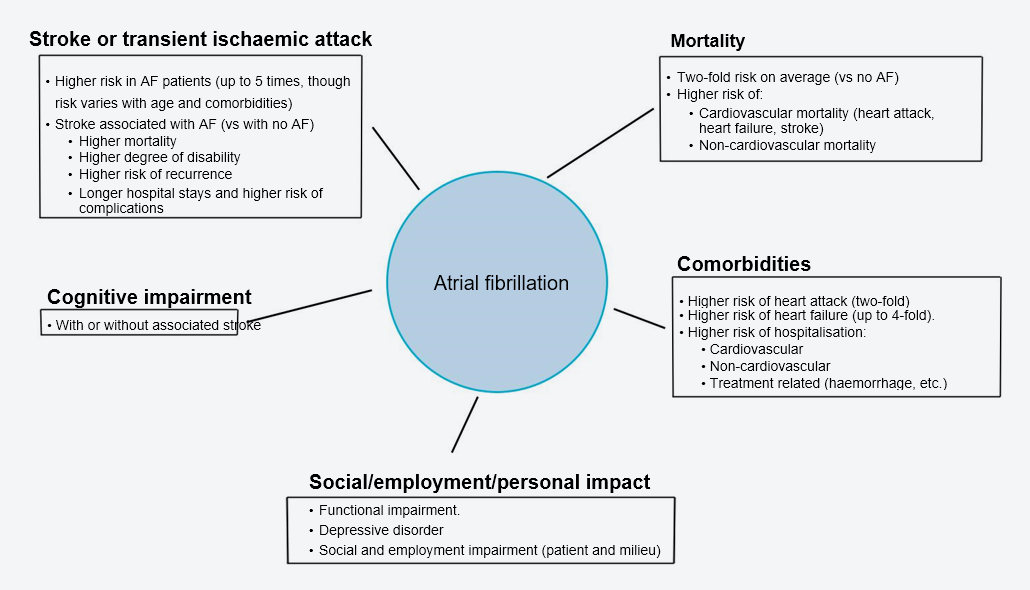
Figure 17. Most frequent complications of AF.
Source: Revista Española de Cardiología. 2021; 21 Suppl. A: 9-17.
Oral anticoagulant therapy is indicated in AF patients who suffer from an additional condition listed by the CHA2DS2-VASc scale. Direct oral anticoagulants (DOACs) have a predictable, linear, non-fluctuating anticoagulant effect, eliminating the need for regular anticoagulation monitoring and frequent changes in dosage. Furthermore, on the whole they are also more effective in preventing thromboembolic complications and have a lower risk of intracranial haemorrhage, hence mortality tends to be lower than with non-vitamin K anticoagulants (1) (NOACs) like warfarin (2) (Figures 18 and 19).
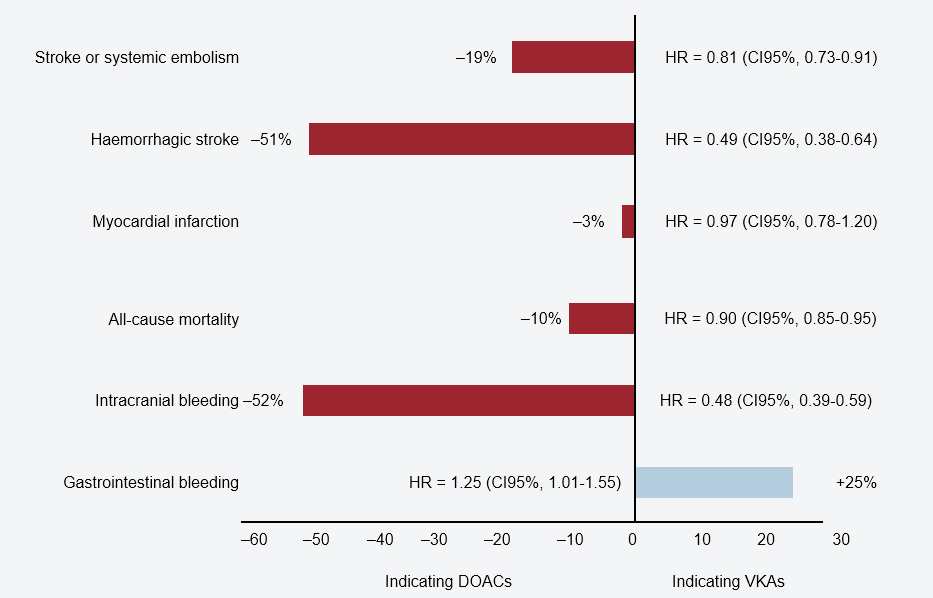
Figure 18. Efficacy and safety of direct oral anticoagulants vs warfarin. Clinical trial meta-analysis. HR: hazard ratio; CI95%: 95 % confidence interval.
Source: Revista Española de Cardiología. 2021; 21 Suppl. A: 9-17.
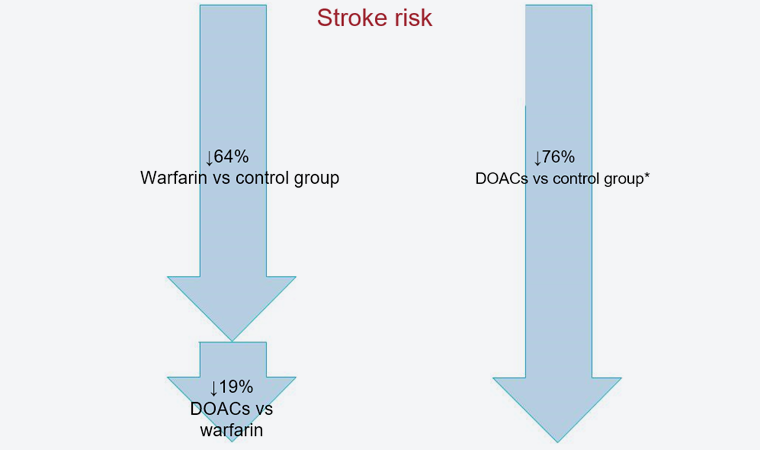
Figure 19. Stroke risk reduction using oral anticoagulants. *Estimate vs control group.
Source: Revista Española de Cardiología. 2021; 21 Suppl. A: 9-17.
The CHA2DS2-VASc score should therefore be used for AF patients. This scale is used internationally as a measure of the risk of thromboembolism and stroke in atrial fibrillation patients (Figure 20).
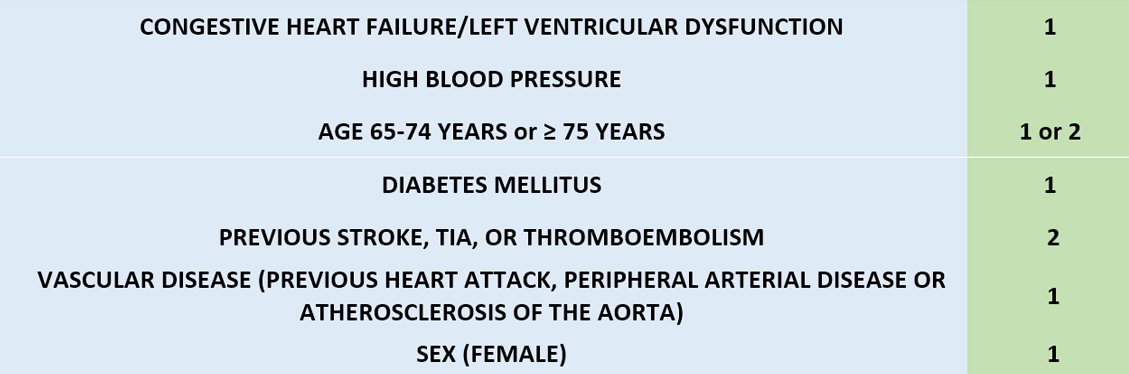
Where "yes" = 1 and "no" = 0 points (except age >75 and stroke, TIA, or previous thromboembolism = 2 points)
The score of from 1 to 9 points indicates the risk category and percentage risk of suffering a cerebrovascular accident (stroke) per year.
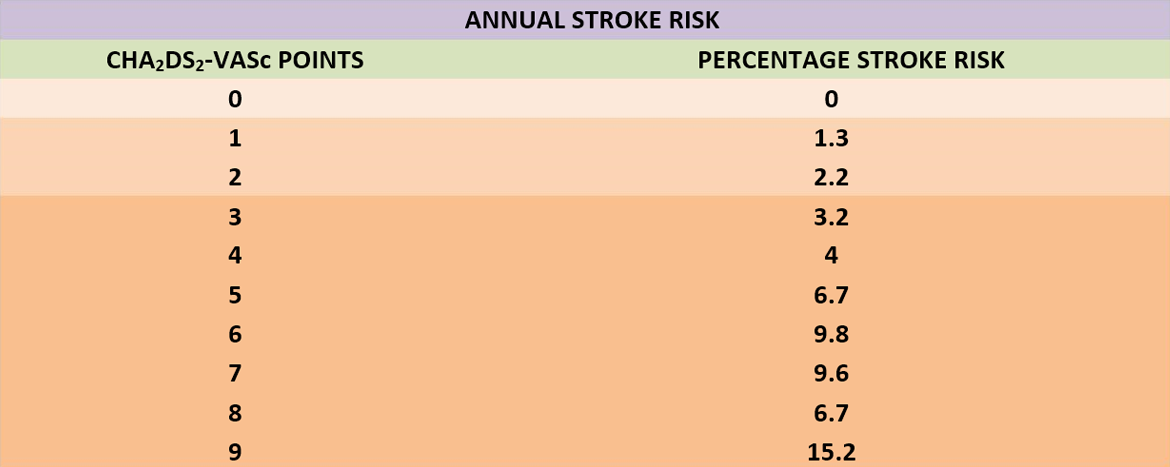
Used to decide whether or not the patient requires treatment with anticoagulants or antiaggregants. The table that follows sets out treatment recommendations according to the CHA2DS2-VASc score in patients with atrial fibrillation.
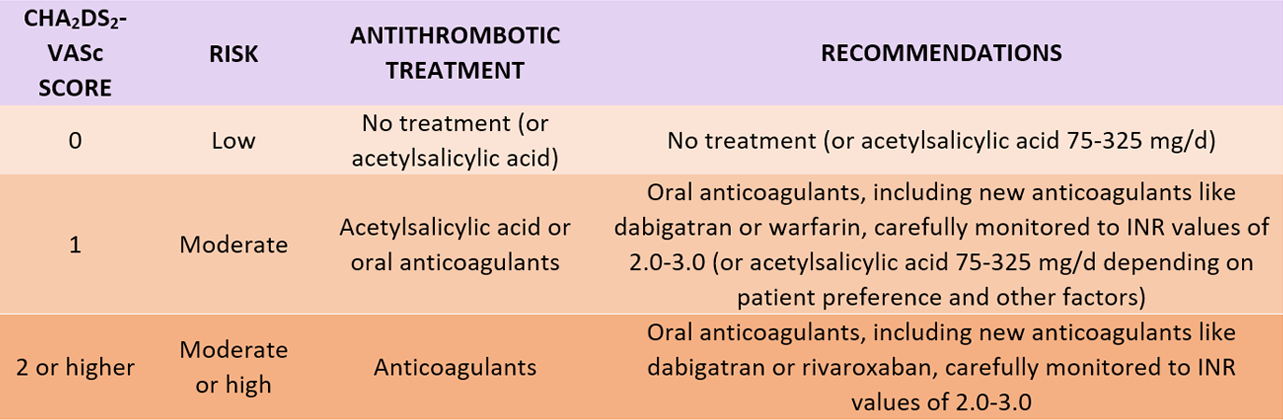
Figure 20. CHA2DS2-Vasc Score.
Source: https://1aria.com/images/entry-pdfs/escala-cha2ds2-vasc.pdf.
Cardiovascular risk is the probability of suffering CVD within a certain time window. Accordingly, cardiovascular risk assesses cardiovascular mortality, the set of all fatal and non-fatal cardiovascular complications, myocardial ischaemia complications, both objective complications like acute myocardial infarction and subjective complications like angina pectoris, cerebrovascular complications, etc. Current CVD prevention recommendations emphasise multifactorial risk assessment to arrive at integrated prevention advice for patients. Estimating a person's cardiovascular (CV) risk or coronary disease (CD) risk is an essential tool for clinical decision-making on the interventions needed to bring risk factors under control.
Various scales for quantifying cardiovascular risk have been developed. Their differences lie not only in the two variables mentioned above, which CVD is being considered over which time interval, but also in the specific parameter values used in the calculations. These parameters have traditionally been known as risk factors. Their relationship to subsequent CVD incidence has been established for different derivation cohorts, i.e., the populations used to compile risk factor and CVD data, and then plotting time trends. The algorithms thus obtained are checked for those same populations or preferably against other populations called validation cohorts.
The first and second European preventive Task Forces used a chart for estimating coronary risk based on 12 years of follow-up of a combination of the original Framingham cohort and the cohort of their offspring, 5,573 people in all. However, the resulting function was observed to overestimate CD risk in various European populations. The third joint CD prevention Task Force instead recommended using the SCORE (Systematic Coronary Risk Evaluation) system in clinical practice. SCORE estimates the 10-year risk of death from CD based on age, sex, systolic blood pressure, total blood cholesterol, and smoking based on 12 studies of European cohorts totalling 205,178 subjects (43% women) ranging in age from 24 to 75.
Asymptomatic Spaniards between 40 and 74 years of age with a 5% risk and thus candidates for intensive counselling are estimated to number in excess of 3 million. This figure does not include others at high risk who have just a single very elevated factor, namely, high blood pressure of 180/110 mm Hg, or elevated total cholesterol, or cholesterol plus elevated low-density lipoproteins (LDL cholesterol). If these are counted, the number of candidates for personalised intervention was 4,646,896 (3,029,913 men, 1,616,983 women) in 2002, plus patients already diagnosed with CVD previously.
These are findings of the SCORE CVD risk scale's calibration study for Spain prepared by the Instituto de Estudios de la Salud [Health Studies Institute] in Barcelona in association with the University College Cork's Department of Epidemiology and Public Health in Ireland, the Royal College of Surgeons' Department of Epidemiology and Public Health Medicine, and the Adelaide and Meath Hospital's Cardiology Service, both in Dublin, Ireland. As in other countries, the size of the population of candidates for intensive intervention is quite large, which is not surprising, since cardiovascular diseases are the leading cause of death, hospitalisation, doctor's visits to primary care physicians, and healthcare expenditures worldwide. That is why it is important to take up to date organised preventive measures to keep a health problem that affects a large section of society under control.
At the same time, prevalence of AF is over 4% of the population aged 40 and over. The prevalence of AF has been observed to be rising in the developed countries and is expected to double in Spain in the coming decades as the population gradually grows older, survival rates for CVD patients improve, and AF-related risk factors, obesity in particular, increase.
Using statistics-based predictive analytics and new computer modelling technologies, Big Data, and Machine Learning capable of extracting and generating data and identifying risks and opportunities is extremely helpful.
First, the ability to make projections that enable us to forecast the future from a preventive medicine perspective and in that way embark on a paradigm shift towards personalised precision medicine to diminish morbidity and mortality and decrease adverse social impacts.
Second, the ability to reduce claim rates and lower the cost per claim to health insurance companies (medical and surgical healthcare costs). Third, the ability to lower the social cost of public health demands caused by the incapacitating sequelae of ischaemic heart disease (heart attack) and neural conditions from haemorrhagic or ischaemic stroke.
It should be noted that approximately 80% of cardiovascular diseases are preventable and can be delayed by a healthy lifestyle and by rushing to the hospital on observing any warning symptom like chest pain caused by ischaemic cardiac disorders (angina and heart attack) and neurological alterations from cerebrovascular disorders (stroke). Response times are critical and decisive to subsequent evolution of patients with these two disorders, with respect to both mortality and incapacitating sequelae (morbidity).
However, there is still much work to be done in the areas of awareness raising, health education, and preventive public cardiovascular medicine to increase participation by citizens, encouraging people to take a much more proactive role in preventive cardiovascular and cerebrovascular diseases, change their eating habits and lifestyle, and increase their physical activity and daily exercise. This is the only way we will be able to reduce both morbidity and sequelae and the resulting high mortality.
Assmann, G.; Cullen, P. & Schulte, H. Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the prospective cardiovascular Munster (PROCAM) study. Circulation. 2002, 105 (7), 310-315.
https://doi.org/10.1161/hc0302.102575
Alegría, E.; Alegría, A. & Alegría, E. Estratificación del riesgo cardiovascular: importancia y aplicaciones. Revista Española de Cardiología, 2012, 12 (C), 8-11.
https://doi.org/10.1016/S1131-3587(12)70039-0
Benjamin, E.J.; Wolf, P.A.; D’Agostino, R.B.; Silbershatz, F.A.; Kannel, W.B. & Levy, D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998, 98 (10), 946-952.
https://doi.org/10.1161/01.cir.98.10.946
Berger, J.S.; Jordan, C.O.; Lloyd-Jones, D. & Blumenthal, R.S. Screening for cardiovascular risk in asymptomatic patients. Journal of the American College of Cardiology. 2010, 55 (12), 1169-1177.
https://doi.org/10.1016/j.jacc.2009.09.066
Catapano, A.L.; Reiner, Z.; De Backer, G.;Graham, I.; Taskinen, M.R.; Wiklund, O.; et al.
ESC/EAS Guidelines for the management of dyslipidaemias: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Atherosclerosis. 2011, 217 (1 Suppl 1), S1-S44.
https://doi.org/10.1016/j.atherosclerosis.2011.06.012
Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G. & et al. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. European Heart Journal. 2003, 24 (11), pp. 987-1003.
https://doi.org/10.1016/s0195-668x(03)00114-3
Cooney, M.T.; Cooney, H.C.; Dudina, A. & Graham, I.M. Total cardiovascular disease risk assessment: a review. Curr Opin Cardiol. 2011, 26 (5), 429-437.
https://doi.org/10.1097/HCO.0b013e3283499f06
Daiichi Sankyo. We Care for Every Heartbeat. 2022.
Disponible en: https://www.daiichi-sankyo.es/cardiovascular/we-care-for-every-heartbeat/
D’Agostino, R.B.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M. & et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. 2008, 117 (6), 743-753.
https://doi.org/10.1161/CIRCULATIONAHA.107.699579
Freixa-Pamias, R.; Pérez A.I.; Valle, A. & Fernández, I. Impacto de los cambios en la prescripción del tratamiento anticoagulante en la incidencia de ictus. On: Protección contra el ictus relacionado con la fibrilación auricular en la era de la COVID-19: Retos y necesidades. Revista Española de Cardiología. 2021, 21(A), 19-21.
https://doi.org/10.1016/S1131-3587(21)00003-0
Gómez-Doblas, J.J.; López-Garrido, M.A.; Esteve-Ruiz, I. & Barón-Esquivias, G. Epidemiología de la fibrilación auricular. Revista Española de Cardiología. 2016, 16 (A), 2-7.
https://doi.org/10.1016/S1131-3587(16)30007-3
Guize, L.; Thomas, F.; Bean, K.; Benetos, A. & Pannier, B. Atrial fibrillation: prevalence, risk factors and mortality in a large French population with 15 years of follow-up. Bulletin de l´Académie Nationale de Médecine, 2007, 191 (4 Suppl 5), 791-803.
Heering, J.; Van der Kuip, D.; Hofman, A.; Kors, J.A.; Van Herpen, G.; Stricker, B.H. & et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study.
European Heart Journal. 2006, 27(8), 949-953.
https://doi.org/10.1093/eurheartj/ehi825
Hippisley-Cox, J.; Coupland, C.; Vinogradova, Y.; Robson, J.; Minhas, R.; Sheikh, A. & et al. Predicting cardiovascular risk in England and Wales: prospective derivation and validation of QRISK2. BMJ. 2008, 336 (7659), 1475-1482.
https://doi.org/10.1136/bmj.39609.449676.25
Kannel, W.B.; Wolf, P.A.; Benjamin, E.J. & Levy, D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. American Journal of Cardiology. 1998, 82 (7 Suppl 1), 2N-9N.
https://doi.org/10.1016/s0002-9149(98)00583-9
Masjuan, J.; Cequier, A.; Expósito, V.; Suárez, C.; Roldán, I.; Freixa-Pamias, R. & et al. Prevención del ictus en pacientes con fibrilación auricular. Mejorar la protección en la era de la COVID-19. In: Protección contra el ictus relacionado con la fibrilación auricular en la era de la COVID-19: Retos y necesidades. Revista Española de Cardiología. 2021, 21(A), 9-17.
https://doi.org/10.1016/S1131-3587(21)00002-9
Meza-Miranda, E.A.; Romero-Espínola, N. & Báez Ortiz, E.A. Factores de riesgo modificables de enfermedad cerebrovascular en pacientes que han sufrido un ictus.
Revista de Nutrición Clínica y Metabolismo. 2021, 4 (4), 24-31.
https://doi.org/10.35454/rncm.v4n4.317
Morillas, P.; Pallarés, V.; Fácila, L.; Llisterri, J.L.; Sebastián, M.E.; Gomez, M. & et al. La puntuación CHADS2 como predictor de riesgo de ictus en ausencia de fibrilación auricular en pacientes hipertensos de 65 o más años. Revista Española de Cardiología. 2015, 68 (6), 485-491.
https://doi.org/10.1016/j.recesp.2014.06.028
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002, 106 (25), 3143-3421.
Nordestgaard, B.G.; Chapman, M.J.; Ray, K.; Borén, J.; Andreotti, F.; Watts, G.F. & et al. Lipoprotein(a) as a cardiovascular risk factor: current status. European Heart Journal. 2010, 31 (23), 2844-2853.
https://doi.org/10.1093/eurheartj/ehq386
Perk, J.; De Backer, G.; Gohlke, H.; Graham, I.; Reiner, Z.; Verschuren, M.; et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). European Heart Journal. 2012, 33 (13), 1635-1701.
https://doi.org/10.1093/eurheartj/ehs092
Pérez-Villacastín, J.; Pérez-Castellano, N. & Moreno-Planas, J. Epidemiology of atrial fibrillation in Spain in the past 20 years. Revista Española de Cardiología. 2013, 66 (7), 561-565.
https://doi.org/10.1016/j.rec.2013.02.012
Ridker, P.M.; Buring, J.E.; Rifai, N. & Cook, N.R. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the Reynolds Risk Score. JAMA. 2007, 297 (6), 611-619.
https://doi.org/10.1001/jama.297.6.611
Ridker, P.M.; Paynter, N.P.; Rifai, N.; Gaziano, J.M. & Cook, N.R. C-reactive protein and parental history improve global cardiovascular risk prediction: the Reynolds Risk Score for men. Circulation. 2008, 118 (22), 2243-2251.
https://doi.org/10.1161/CIRCULATIONAHA.108.814251
Sans, S.; Fitzgerald, A.P.; Royo, D.; Conroy, R. & Graham, I. Calibración de la tabla SCORE de riesgo cardiovascular para España. Revista Española de Cardiología. 2007, 60 (5), 476-485.
https://doi.org/10.1016/S0300-8932(07)75064-9
Wang, T.J.; Larson, M.G.; Levy, D.; Vasan, R.S.; Leip, E.P.; Wolf, P.A. & et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation. 2003, 107 (23), 2920-2925.
https://doi.org/10.1161/01.CIR.0000072767.89944.6E
Wilson, P.W, D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H. & Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation. 1998, 97 (18), 1837-1847.
https://doi.org/10.1161/01.cir.97.18.1837
Woodward, M.; Brindle, P. & Tunstall-Pedoe, H. Adding social deprivation and family history to cardiovascular risk assessment: the ASSIGN score from the Scottish Heart Health Extended Cohort (SHHEC). Heart BMJ Journals. 2007, 93 (2), 172-176.
https://doi.org/10.1136/hrt.2006.108167
World Health Organization. Las 10 principales causas de defunción. 2020. Available on: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death

Dr. Javier Cabo Salvador, Medical Doctor and Doctor in Cardiovascular Surgery. Director, Department of Health Science, Chair in Health Management and Health Science, UDIMA [Madrid Distance Learning University], Chair in Biomedical Engineering, Catholic University of Murcia (UCAM), and Chair in Biomedical Research, Catholic University of Nordestana (UCNE), Member of BIONECA (Biomaterials and Advanced Physical Techniques for Regenerative Cardiology and Neurology). Member of the New York Academy of Sciences. Managing Director of Medytec Salud, Groupama Plus Ultra (currently Catalana de Occidente)'s healthcare management company 2000-2010. Head of Cardiovascular Surgery, La Paz University Hospital (1990-2017).